In the first year of the pandemic, there were many types of sign associated with Covid-19: warning signs; names; national symbols; new indicators for numbers and trends; orders; images; and instructions. However, when I wrote about Covid-19 and signs in 2020, I failed to predict the dominance of a particular type of sign in responses to the pandemic: group signs or signs for a particular group within a population (‘people at higher risk‘) or for a population as a whole but viewed in a particular way (‘global excess morbidity‘).
In its second year, responses to Covid-19 turned to living with an endemic disease and to developing fluid strategies to control infections, deaths and pressure on health care services. There were some exceptions to ‘living with’ strategies, such as New Zealand, though gradually zero-Covid strategies were abandoned. Irrespective of their exact form, these strategies drove the turn towards group signs.
In this post, I will argue that these strategies and their presuppositions in relation to group signs require critical review because such signs always have political presuppositions and implications. My analysis will focus on epidemiology, as a forecasting science at the forefront of advice to governments. The groups concerned include nations and sections of populations identified in terms of disease prevention. They have been central to strategic advice and reversals of advice; for instance, through confinement, vaccination and travel bans.
In terms of reversals in forecasts and policies, and as an example of a group sign defined around a nation, in July 2020 Professor Devi Sridhar, Chair in Global Public Health and Scottish Government Covid-19 Advisory Group member, and Dr Adriel Chen ‘looked at how Scotland was on course to eliminate the virus’. It wasn’t. Here is the graph of Covid-19 cases and deaths in Scotland after July 2020.
This is not to say that epidemiological forecasting for Scotland is poor, but rather that it is representative not only of the difficulties in forecasting for epidemiological science during an ongoing pandemic, but also of the risks and effects of strategic thinking dependent on group signs.
There are good reasons for the scientific reversal, such as different policy decisions and new variants, but the use of a group sign like ‘Scotland’ (the population within the boundaries of Scotland) introduces political and philosophical complexities and consequences that take epidemiology beyond the boundaries of natural science into social sciences and politics. This undermines the distinction drawn between science and non-science during the pandemic.
Professor Sridhar blamed the failure on opening Scotland’s borders and the B.1.1.7 variant. Scotland’s borders were never closed. It would have been extremely difficult to do so, given essential and continuing traffic with England along five main arteries and a great many minor roads and the lack of any border infrastructure on any of them.
The group sign ‘Population within Scotland’s borders’ is easy to coin and use. It has an air of objectivity. Nonetheless, it is also a complex political sign, resistant to easy delineation. It implies sweeping legal and policing measures, if it is to correspond to a truly confined population.
Measures would have had to be stronger than the political theatre of the largely unenforceable ban on travel from Manchester to Scotland in June 2021, where there were no road blocks or systematic checks on the busy M6/M74 corridor. During stricter Australian lockdowns and corresponding state border rules, a single removal lorry crew spread the Delta Covid-19 variant from New South Wales to multiple sites in Victoria. In the eight days of the attempted Scottish travel ban on areas of Manchester, thousands of lorries and cars crossed daily from England unchecked.
More virulent variants were part of the forecasting models, but their spread was dependent on the success of ongoing public health measures and on the success of border closures, internal travel bans and lockdowns. This created a feedback loop with political and social factors, making forecasting uncertain and reliant on the success of public health measures.
Fatigue and disobedience can grow in a pandemic, thereby requiring new and experimental models sensitive to them. This responsiveness can only be partly successful, since exhaustion and rebellion are themselves reactive to changes in political force and type, to different degrees and in unpredictable ways. This unpredictability with respect to order and disorder can be seen in another recent political context with poor forecasting, not only of the onset of the Arab Spring, but also of its waning and eventual suppression.
Any review of epidemiology and the pandemic will therefore have to consider the presuppositions of epidemiology in terms of government, political systems and language. How do models assume forms and degrees of political power? Do they take account of geographical, economic and social difficulties that may influence social behaviour and political decisions? What do the elements of these models, defined by group signs, imply not only for strategies but also for their effects?
The first thing to note is how the statement of a group sign such as ‘We should protect others‘ can be far-removed from its application. It was striking that in England and in Scotland leading advisors, officials and politicians failed signally to follow the advice they imposed on others. Politicians and scientific advisors applied models at odds with their behaviour. A more truthful, but perhaps less convincing group sign would have been (and perhaps still is) ‘You should protect others, even if we do not‘.
During the pandemic, strong distinctions have been drawn between science and politics (‘We follow the science‘). Yet, given its necessary presuppositions about politics, every time epidemiology uses a group sign such as ‘the population of Western Australia’, ‘we’, ‘that nation’, ‘this island’, ‘that subsection of the population’ or ‘the implementation of this policy here‘, it is partly a political science creating and reinforcing different political signs, policies, categories, values, judgements and systems.
A lockdown might well be indicated by scientific models, but its success and hence the models themselves involve assumptions about how a population can be encouraged or made to comply. The same is true for monitoring measures, some of which are highly intrusive, repressive and reinforcing of trends towards the systematic technological control of populations.
Epidemiology depends on ideal models of polity, when it models for degrees of political compliance by populations as they respond to a great range of changeable and changing types of political leadership, coercion and persuasion. For instance, mathematical models for behaviour in a pandemic make assumptions about rational choices and about reactions to changes in links in transmission networks:
On closer inspection, the models that assume a changing network structure generally make two assumptions about how the transmission network changes. First, an existing link is removed. In practice, this is a possibility only in cases where the wish to distance oneself from the infection overrides the reasons for the existence of the transmission link in the first place… Some of the models go one step further and assume that after a link has been removed, a new one is formed (link rewiring) with a random new contact. For such rewiring to have an effect on infectious disease dynamics, the rate of change to the network would need to be of a similar magnitude as the spread of disease which is often not the case. More importantly, however, based on the available evidence on social network formation in humans, random link formation is of limited importance in network structure evolution. Thus, in our view, current models that take into account a change in the network structure can only be applied with great caution to infectious diseases in humans.
https://royalsocietypublishing.org/doi/10.1098/rsif.2010.0142#d3e478
Against my argument that every idealisation is itself political, it could be objected that these assumptions are about mathematical models and accurate empirical observation. The mathematics have to be correct – for instance about equilibria in decision making – and empirical observations should support the assumptions about behaviour. However, as the cited article points out, evidence is scant and unreliable (in 2010 and still now). Furthermore, behaviour depends on which political systems influence and control it. These systems adapt to behaviour and innovate to influence it. It is not only that evidence is scant. It’s that it is rapidly changing and highly variable, depending on where it has been gathered and when.
Early on in the pandemic, a report in Science on the success of China in controlling a Covid-19 outbreak drew attention to the tension between advocating a policy and supporting the political system leading to its success: ‘The question now is whether the world can take lessons from China’s apparent success—and whether the massive lockdowns and electronic surveillance measures imposed by an authoritarian government would work in other countries.’
As Professor Sridhar points out in the report, praising that success is also to gloss ‘over the whole human rights dimension’. That’s to put things mildly. The China successful at suppressing the Covid-19 outbreak (at a particular time) is also the China repressing democracy movements in Hong Kong. Many of the features of Chinese polity, such as very tight monitoring of citizens, the ability to curtail rights rapidly and oppressive control over information are shared between control of the pandemic and repression of counter-movements, dissent and minorities.
In endorsing the success of, say, China or New Zealand or India or Portugal or Israel or Australia or the World Health Organisation, epidemiologists are also endorsing and recommending political systems, types of border and forms of communication, control, punishment and reward – at a given time and subject to often extreme reversals over time. To recommend Singapore’s ‘pandemic response model’ is to recommend a model leading to deep iniquities.
The following passage from an abstract on ‘lessons in global health governance’ in Nature exhibits these political tensions, in this case between WHO and nation states: ‘The World Health Organization has played a pivotal technical, normative and coordinating role, but has been constrained by its lack of authority over sovereign member states. Many governments also mistakenly attempted to manage COVID-19 like influenza, resulting in repeated lockdowns, high excess morbidity and mortality, and poor economic recovery.’
Irrespective of whether the WHO gave good or bad advice when declaring a pandemic, advising against travel, communicating about the dangers of Covid-19 and advocating for vaccines and sharing them, its constitution and relation to member states was such that they frequently did not listen. In that sense, it is a stretch to claim the WHO had a pivotal role. The claim works better if read as the WHO should have had a pivotal role, but that is a political claim as well as a medical one, because it concerns the constitution and reach of international organisations.
The linked document is an internationalist political statement rather than a straightforwardly scientific one. From a political science point of view, it ignores or underplays questions about contemporary shifts away from multilateralism, the recent checkered history of UN and WHO interventions in Haiti, Bosnia and Congo, scepticism towards enlightenment values, Western universalism, and the influence and motivations of multinationals, billionaires and ex-politicians with dubious claims to moral leadership on global matters.
Group signs are the medium through which these political presuppositions are articulated. They are the condition for identifying nations, populations, political entities and subsections of populations. My main point is that whenever a group sign is used, there are necessarily political implications and assumptions. The political dimension of epidemiology is therefore unavoidable and the critical question is then not about how to avoid them, but how to draw them out, reflect upon them and select them well. This selection is all-important. My claim isn’t that all political assumptions are equivalent. It’s that they are unavoidable and we need to investigate what they are and which we should adopt (with caution and constant review).
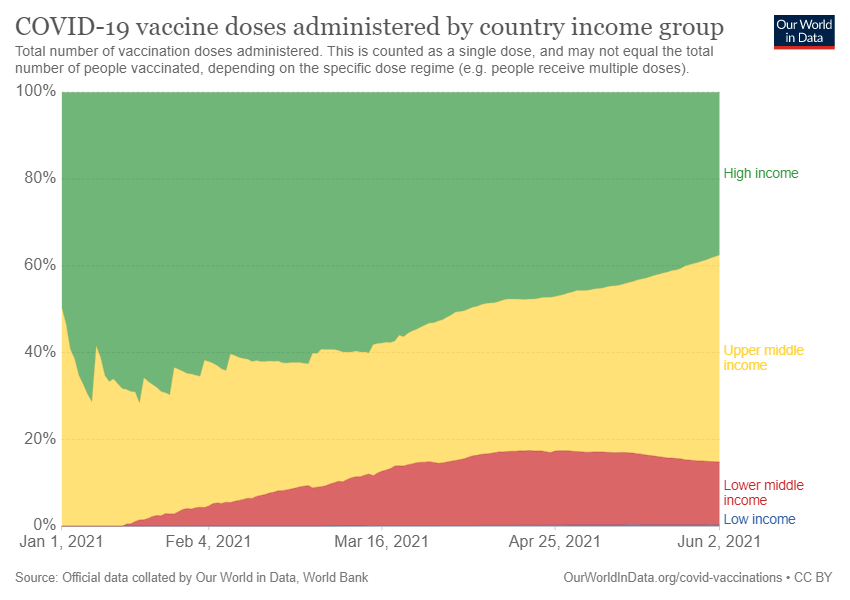
The bands in the chart at the start of this post are group signs. They divide world populations according to income. In terms of access to the vaccine, there is a stark divide; some rich countries are deploying booster vaccine jabs when others have not been able to afford to protect even their most vulnerable. Underlying this split into groups, there is the currently dominant group distinction and political flashpoint: vaccinated or unvaccinated (for instance, with Austria introducing lockdown for the unvaccinated).
I called Covid-19 strategies ‘fluid’ earlier to highlight two points. First, the strategies cope with a changing situation, notably in terms of new variants of the virus and in terms of the ebb and flow of the disease according to looser and stricter control measures. Second, though we often think of strategies as methods to achieve a goal, a strategy is a two-way process connecting problems to responsive strategies. The goal keeps moving, because it is generated by a dynamic and complex problem with natural, social, environmental, economic, political and ethical parameters.
The strategies for Covid-19 are about population management in a dynamic and complex situation. They focus on indicators, aims and actions: What’s happening? What should we do? How should we do it? Group signs indicating who is at risk, or where we should focus our resources, or how we should make a population comply are therefore central to the management of the spread of the virus and of its effects. The problem is that group signs also carry risks.
Group signs are intrinsically inaccurate. They collect many different people under a single banner, like an average, a threshold, or a general characteristic with wide variations. They also introduce rough distinctions across populations. For instance, the shorthand ‘old’ and ‘young’ not only depends on which population, where and when, but also invites false inferences based on different concepts of youth and age. In the early days of the pandemic, there was a dangerous conclusion that the advanced age and comorbidities of many of the victims meant they were likely to have died soon anyway. The conclusion was false.
Groupings are also prone to secondary consequences that can inhibit a strategy; for instance, when a group is excluded, victimised or demonised. I will give two examples of these risks – one egregious, the other more subtle – about war and about intentions, prior to setting out the general form for group signs explaining why they should always be treated with caution.
For the current crisis, responses have sometimes been couched in the language of war, thus making the problem about an ‘enemy’ – one of the most inaccurate, misleading and destructive group signs. With its militaristic meanings, war is an inadequate context for the challenge of endemic disease, not least because, for different groups, it imports the moral values of war iconography (courage and cowardice, strength and weakness, good and evil, innocent and combatant) into processes based on biology, luck and social factors (it is far worse luck to be born poor in the age of Covid-19).
When we discuss how to tackle the pandemic as a war between opposed groups, we transfer the language of war to populations. Different people become enemy combatants, traitors, allies, courageous fighters, or cowards. This analogy reached abject levels in the attribution of signs and ideas from the Third Reich to different “sides” in debates about vaccination and policies such as passes controlling entry to places where the virus spreads more easily.
In France, demonstrators called for resistance to what they called a Nazi policy – health passes indicating vaccination, a recent negative test or past infection, for access to restaurants, cinemas, some transport and hospitals for non-urgent interventions or visits – a few metres away from memorials to resistance fighters, deported Jews and civilians assassinated by German troops and the Gestapo.
Every town and village in France has memorials to the horrors of war, yet in France and elsewhere during the pandemic, the language of war and resistance has been adopted in dismal ignorance of the past, often by politicians claiming to be speaking for some precious and lost nation, but also by governments and scientists repeating the crude violence of easy distinctions between sides in a war.
Group signs about wars, let alone wars against a virus and between opponents in strategies for overcoming Covid-19 invariably miss the individual and collective poignancy of war memorials, with their precise dates, reference to specific horrifying events and lists of the fallen. These are multifaceted signs calling for remembrance of what wars – and talk of war – lead to.
Attributing warlike aims to the virus is also a fallacy (the virus does not aim to kill us). Attributing any aim to the virus is a mistake, when compared to describing what it does rather than what it intends to do. If we think of intentions, we also assume there is an intending consciousness or a valid analogy with intentions: the virus as subject of an aim. This is a misrepresentation of the random evolution of the virus; a misunderstanding reinforcing the common belief that the occurrence of variants in a circulating virus is rare and purposive when the opposite is the case.
The question of intentions in response to Covid-19, introduces another deceptive distinction through group signs: between ‘chose to be vaccinated’ and ‘chose not to be vaccinated’. According to the assumption of intention, vaccine adoption and hesitancy are approached primarily as reasoned choices with intended outcomes. The presupposition of freedom is key here. I’ll highlight its pitfalls and negative consequences in terms of judgements and understanding of the pandemic.
First, intentions are a distraction because they concentrate attention on unreliable evidence. It is far less helpful to predict or forecast the behaviour of human populations on the basis of what interviewees say they intend to do than on the basis of what they have done and currently do.
We should prioritise verified statistics over polls about future intentions. The former are more robust indicators. Respondents say they will behave in a certain way, but that’s often based on misunderstandings and therefore either unstable in relation to new information (and can be corrected by understanding) or unstable due to irrational beliefs (and can’t be corrected easily by well-supported information yet can still change rapidly).
When compared to death rates as measured by actuaries general beliefs about the mortality of Covid-19 in 2020 were unreliable and unstable. Yet these beliefs formed the basis for reported intentions about future behaviour. These beliefs and intentions changed rapidly, as shown for example by big shifts in attitudes to vaccination in France (the link is to an industry funded site, but what it reports is confirmed across many other sources).
The dismal performance of polling in recent elections should be a stark warning against reliance on stated intentions in the much more difficult question of behaviour in a new pandemic. It is not what we say about what we might do in future that matters. It’s what we do and have done.
Intentions are conditional and thereby uncertain when compared to past acts. When we rely upon stated intentions, we overemphasise a supposedly free decision that comes with unsaid conditions many of which are unknown at the time (but I won’t do it if that happens, or if “something else” happens). The fast-changing nature of a novel pandemic will generate many such conditions. These provisos and uncertainties can be observed by studying historical cases and theories of – for instance – the contagiousness of emotions in the pandemic where rapid shifts in emotions bring about pronounced changes in attitudes.
Second, when good and bad things have happened to individuals or groups, it is inaccurate and unfair to judge them on the basis of their free intended acts, compared to an understanding of other causes. For instance, attributing differing vaccination rates to free intentions is inaccurate, when there are other circumstances offering much better explanations for variations in uptake.
Individuals and populations react according to a wide range of deep-rooted causes, such as negative historical experiences. The linked paper is reporting on intentions, but these are explained according to deep-seated reasons that cannot be assumed to be easily replaced by a different free decision. For instance, past experiences and other structural factors explain poor vaccination rates in Guadeloupe influenced by poor healthcare, mistrust of the metropole and the chlordécone scandal. Here, the idea of free, poorly conceived and blameworthy decisions made by independent subjects is incorrect and unjust.
Third, we shouldn’t see ourselves as absolutely free, but rather as effects of influences making us only relatively free. This might appear paradoxical, since the phrase ‘what we should do’ implies a freedom to intend to do one thing or another. However, there is a different sense of freedom between a decision to act within wider constraints and the assumption that we can act completely freely when we intend to do something.
For the pandemic, the importance of the distinction between limited and absolute freedom lies in how we consider and address populations. If there are absolutely free intentions, irrespective of actual limitations thereafter, then we should consider populations as equivalent in the power to choose. We can have a single correct argument that we expect individuals to bend to, or be blamed if they don’t.
However, if there are limited and conditional decisions, then we should consider how any given group is conditioned and limited. Our arguments must then address those reasons and it is wrong and ineffective to expect assent to universal arguments and apportion blame when they aren’t followed. The current distinction between two groups according to intentions gives a false picture.
The lesson from signs such as ‘enemy’ or ‘vaccine hesitant’ is that while they might serve to identify a group to be considered in controlling or treating Covid-19, this comes at a cost to be taken into account before signs are put to use.
Group signs divide populations into distinct categories, such as age (’60-70′), specific features (‘vaccinated’, ‘at risk’), groups determined by boundaries (‘New Zealand’, ‘North-South’), groups defined by activities (‘medical staff’, ‘police’), groups defined by positions or beliefs (‘anti or pro-vaccine’), groups positioned within longstanding categories deemed important for problems and strategies (ethnic groups or particular electorates, for instance) and groups defined not by well-defined features but by much more nebulous cultures and characteristics (‘students’, ‘the young’, ‘the old’, ‘the economically active’).
It could be assumed that group signs are to be rejected as detrimental to individuals. We might instead try to use signs that are sets of individuals: {a with b with c…}. There are two reasons this won’t work. The first is practical, since group signs are necessary for dealing with large numbers; a list of individuals quickly becomes unmanageable. The second is theoretical, because group-signs make abstraction possible and thereby allow for reflection on shared features.
Even if new technologies such as facial recognition and faster databases can treat individuals within large populations, the rules applied thanks to those technologies work in terms of group signs; for instance, when allocating an individual identified on CCTV to the group ‘anti-social’ for supposedly deviant behaviour.
The assessment of group signs shouldn’t be based on a prior assumption about the different values of individuals or groups, but on the different – positive and negative – effects of the creation of group-signs. To do this, I’ll study them using the theory developed in A process Philosophy of Signs. This begins with the simple notation for a sign {A} where, in this instance, A is a group.
The token ‘A’ is already political, since inferences, expectations and feelings alter dependent on the name ‘A’. There are different effects between the choices ’60-70′, ‘older people between 60 and 70’, ‘senior citizens’, ‘the older at risk population’, ‘pensioners’ and ‘our elders’. Note that a group also acquires a name over time; for instance, when the press report on research using a shortened name for a scientific category or without explaining a graph (such as logarithmic graph in Covid-19 reporting). The name isn’t fixed, but varies as a sign is put into circulation.
Against appearances, the selection of a raw number (‘over 60’) is also political and inaccurate, calling for more fine-grained and sensitive treatment; for example, given the different outcomes for men and women over 60 when contracting Covid-19. The stakes around naming and selecting groups leads to a first principle when using group signs. Principle 1: the names and boundaries selected for a group will have wide effects, inviting and allowing many inferences. When a group sign is created it is essential to reflect carefully on those names and boundaries, and to continue to do so as they become discussed.
The mere selection of a group isn’t enough for understanding group signs, particularly for capturing the sense of group used in the treatment of populations, such as signs in a pandemic. There, the name for a group ‘A’ is associated with a subset of a population. So a group sign isn’t simply {the young} as in ‘the young’ are suchlike, but rather {the young, this subset of this population}, as in ‘the young in the UK in 2020’ where the UK in 2020 is a subset of global population over time.
This association of name and subset is important because it means group signs involve three processes of distinction: the naming of the group {Brazilian schoolchildren}; the identification of the subset of the population {those attending school in Brazil in October 2020′}; and the separation of that population from everything else (Brazil considered specifically in terms of its population as divided into at school and not at school).
As shown by the brackets in the notation, group signs distinguish the content of the sign from everything outside the sign, outside the brackets. This distinction doesn’t eliminate that background; it is an operation on it and on the group that it distinguishes. The sign and what it distinguishes appear against a background but also separated from it: {A}/background.
This operation against backgrounds has been noticeable in the pandemic, when specific groups have been separated out for special treatment, to the relief, scorn, sympathy, or dismay of other groups. In Scotland, for instance, students bore the brunt of unfair restrictions and blame early on in the pandemic.
These operations of distinction and separation between groups are particularly sensitive and controversial in pandemics given the combination of infectiousness, heightened emotions of fear, and ignorance. The early days of the AIDS/HIV epidemic show the risks and violence of identifying and falsely judging specific groups during a pandemic.
In recent years, group signs have been at the forefront of the mistreatment of refugees, when a very wide range of different people and desperate situations within our societies and their wider political, economic and social networks are separated out and grouped together under value-laden banners such as {migrants} or {economic refugees}.
The operation of distinction for a group sign is a triple cut away from backgrounds. This means the named group is cut away and identified. The subset is cut away away from the population. And the population is cut away from everything else – everything we could have considered in relation to a problem. Recently, one of the groups this has happened to is ‘Unvaccinated and over 65’, cut away from the population of a particular nation at a particular time (France in November 2021), itself cut away from everything else (lives, environments and contexts such as the pre-existing isolation of older adults).
I’ve already given a principle of caution about the naming of group signs. The process of distinction or cut away from a background leads to two further principles. Principle 2: When creating a group sign we should consider the effects and implications of distinguishing a subset of a population from all others. We have seen the risks of that kind of cut in terms of the language of war (identifying enemies, traitors, cowards or collaborators, for instance) and in terms of intentions (falsely identifying a group as simply choosing not to be vaccinated).
Principle 3: When creating a group sign we should consider the wide effects and implications of identifying populations and their subsets, as opposed to connections, continuities, variations and anomalies. The emphasis on distinctions, groups and populations is risky because it divides groups and populations away from other properties and concerns, these might be about individuals or about other types of beings and existence, but in all cases the focus is turned towards what makes a group or a population. In addition to this, differences between groups take on greater significance, not only in terms of how they are different, but also in terms of the consequences of those differences and the values associated with them.
When a group sign is created the following effects necessarily follow:
- A population is drawn out from a wider background
- At least one group is drawn out from that population
- That or those groups are distinguished from all others in the population
These effects aren’t benign since:
- The population is identified at the expense of other things and processes in the background
- The group or groups are identified within the population as having some kind of privileged real existence, as well as positive and negative features
- Stark differences are highlighted and valued at the expense of more subtle continuities and connections
One of the consequences of strategies responding to the Covid-19 pandemic is that group signs have become the dominant way of thinking about our societies. If we do not treat the use of these signs with critical caution, subjecting them to constant review and contrasting them with connections rather than separation, then unjust and violent group distinctions will dominate our lives for much longer than the pandemic.